


Background:
Chronic lymphocytic leukemia (CLL) is the most common adult leukemia in the western world and shows a very heterogeneous clinical course. While the genetic landscape of CLL has been well characterized during recent years it can only partially explain the underlying biology of this heterogeneity. Proteogenomics could offer a valuable tool to fill this gap and improve the understanding of CLL biology.
Methods:
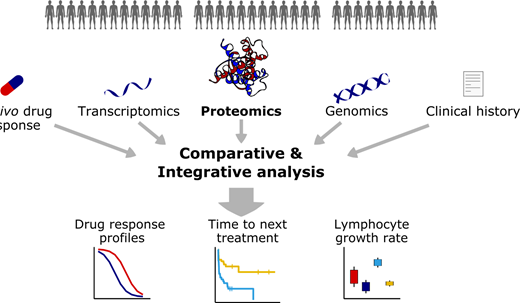
Here, we performed a large proteogenomic analysis (n=263) of three clinically annotated CLL cohorts: For the discovery cohort (Germany_1: n=68) we performed in-depth HiRIEF LC-MS based proteomics (more than 9000 proteins quantified) alongside genome-, transcriptome and ex-vivo drug response-profiling with 43 clinically established drugs. The proteome of two additional validation cohorts (Germany_2: n=44, Sweden_1: n=89), were characterized by data-independent acquisition (DIA) mass spectrometry.
Results:
To connect the CLL genotype with the molecular phenotype, we investigated associations between recurrent genetic alterations of CLL, mRNA expression and protein abundance. We found that trisomy 12, IGHV status and SF3B1 mutations had the greatest impact on protein abundances. CLL specific recurrent chromosomal deletions and gains (trisomy 12, del17p, del13q, del11q, gain8q24) consistently impacted on gene expression and protein abundance through gene dosage effects. We explored functional consequences of these gene dosage effects and found that the additional copy of chromosome 12 increased the abundance of central B-cell receptor (BCR) protein complexes through cis- and trans-effects, which could explain the increased response of trisomy 12 patient samples to BCR inhibition.
Somatic mutations of TP53, ATM and XPO1 were associated with less, but specific and biologically-relevant protein abundance changes. p53 for instance, was the most upregulated protein in TP53 mutated samples, owing to the known stabilisation of mutant p53. This effect was not detectable on transcript level. ATM and XPO1 protein abundances were significantly lower in ATM and XPO1 mutated cases, indicating loss-of-function phenotypes of these mutations.
To understand global similarities and differences between CLL patients on the proteomic level, we performed unsupervised clustering and identified clinically meaningful subgroups. Unsupervised clustering of the proteomics data identified six subgroups with contrasting clinical behaviour. TP53 mutations, IGHV status, trisomy 12 and their interactions explained five subgroups. These results show that quantitative mass spectrometry-based proteomics distinguished clinically relevant subgroups of CLL. Most importantly, we identified a previously unappreciated subgroup of CLL, comprising 20% of all cases, which could be uncovered by proteomic profiling and showed no association with frequent genetic or transcriptional alterations. This new CLL subgroup was characterized by accelerated disease progression, SF3B1 mutation-independent splicing alterations, metabolomic reprogramming and increased vulnerability to inhibitors of metabolic enzymes and the proteasome. Surprisingly, major BCR signaling proteins were downregulated in this subgroup, suggesting less dependence on BCR activity. In accordance with this observation, an unsupervised analysis revealed that low levels of many BCR signaling proteins (e.g. PLCG2 and PIK3CD) were associated with short time to next treatment. The existence of this subgroup could be confirmed in the validation cohorts.
Finally, we performed an unsupervised multi-omics factor analysis (MOFA) across all omics data sets in parallel. This unsupervised analysis confirmed the existence of the above identified CLL subgroups and an important role of SF3B1 mutation-independent splicing alterations in CLL.
Conclusion: Our integrative multi-omics analysis provides the first comprehensive overview of the interplay between genetic variants, the transcriptome, and the proteome, along with functional consequences for drug response and clinical outcome in CLL. Importantly, we identified a new subgroup with accelerated disease progression, a distinct proteomic signature and a clinically exploitable drug sensitivity profile.
Mueller-Tidow:BiolineRx: Research Funding; Daiichi Sankyo: Research Funding; Pfizer: Membership on an entity's Board of Directors or advisory committees, Research Funding; BMBF: Research Funding; Wilhelm-Sander-Stiftung: Research Funding; Jose-Carreras-Siftung: Research Funding; Bayer AG: Research Funding; Deutsche Krebshilfe: Research Funding; Deutsche Forschungsgemeinschaft: Research Funding; Janssen-Cilag Gmbh: Membership on an entity's Board of Directors or advisory committees. Dreger:Neovii: Research Funding; Roche: Consultancy, Speakers Bureau; Riemser: Consultancy, Research Funding, Speakers Bureau; Novartis: Consultancy, Speakers Bureau; Janssen: Consultancy; Gilead: Consultancy, Speakers Bureau; AstraZeneca: Consultancy; AbbVie: Consultancy, Speakers Bureau. Stilgenbauer:Pharmacyclics: Consultancy, Honoraria, Other, Research Funding; Novartis: Consultancy, Honoraria, Other, Research Funding; Mundipharma: Consultancy, Honoraria, Other, Research Funding; Janssen-Cilag: Consultancy, Honoraria, Other: travel support, Research Funding; GlaxoSmithKline: Consultancy, Honoraria, Other: travel support, Research Funding; Gilead: Consultancy, Honoraria, Other: travel support, Research Funding; Genzyme: Consultancy, Honoraria, Other: travel support, Research Funding; Genentech: Consultancy, Honoraria, Other: travel support, Research Funding; F. Hoffmann-LaRoche: Consultancy, Honoraria, Other: travel support, Research Funding; Celgene: Consultancy, Honoraria, Other: travel support, Research Funding; Boehringer-Ingelheim: Consultancy, Honoraria, Other: travel support, Research Funding; Amgen: Consultancy, Honoraria, Other: travel support, Research Funding; AbbVie: Consultancy, Honoraria, Other: travel support, Research Funding. Tausch:Roche: Consultancy, Honoraria, Research Funding; AbbVie: Consultancy, Honoraria, Research Funding; Janssen-Cilag: Consultancy, Honoraria, Research Funding. Dietrich:Roche: Membership on an entity's Board of Directors or advisory committees; Janssen: Membership on an entity's Board of Directors or advisory committees, Research Funding; Celgene: Membership on an entity's Board of Directors or advisory committees; KITE: Membership on an entity's Board of Directors or advisory committees.
This icon denotes a clinically relevant abstract

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal